Occasionally we come across an issue we’ve customarily addressed, but never documented. Put another way: We realize we have a policy – even if an informal one – on how to deal with certain situations, but we’ve never turned that policy into a formal, written one.
It’s incredibly common to have these informal policies in smaller departments, or when a task is rare. You can usually identify them after-the-fact when you are told “That’s just the way we do things here. Everybody knows that.”
When we find these items in our Covered Processes, we should endeavor to document them. Today I’d like to talk about a big one: What do we do when the existing written procedures don’t match with the conditions or situations we are facing in our work. What written guidance are you providing to your Process Operators and Technicians on how to deal with this situation?
Every functioning Operations / Maintenance department has a policy – even if an informal, undocumented one – on how they deal with this issue.
For years I’ve relied on the text in the SOP Written Plan concerning Temporary Operations:
The ammonia system is not operated in any temporary modes without a written SOP. If a component requires maintenance or replacement, that portion of the system is isolated and removed from service through a written SOP. Other Temporary Operations are handled through the MOC element which will ensure supervisory oversight. Temporary Operation SOPs are often via a written modification of an existing SOP in the form of an addendum.
This worked well, but it was a little bit obscure and (understandably) only thought to apply to SOPs themselves. That needed to change. What we’ve done to our system today, is formalized and documented guidance on how to deal with these non-standard / non-routine situations.
A new policy was placed in the RMP Management System Written Plan…
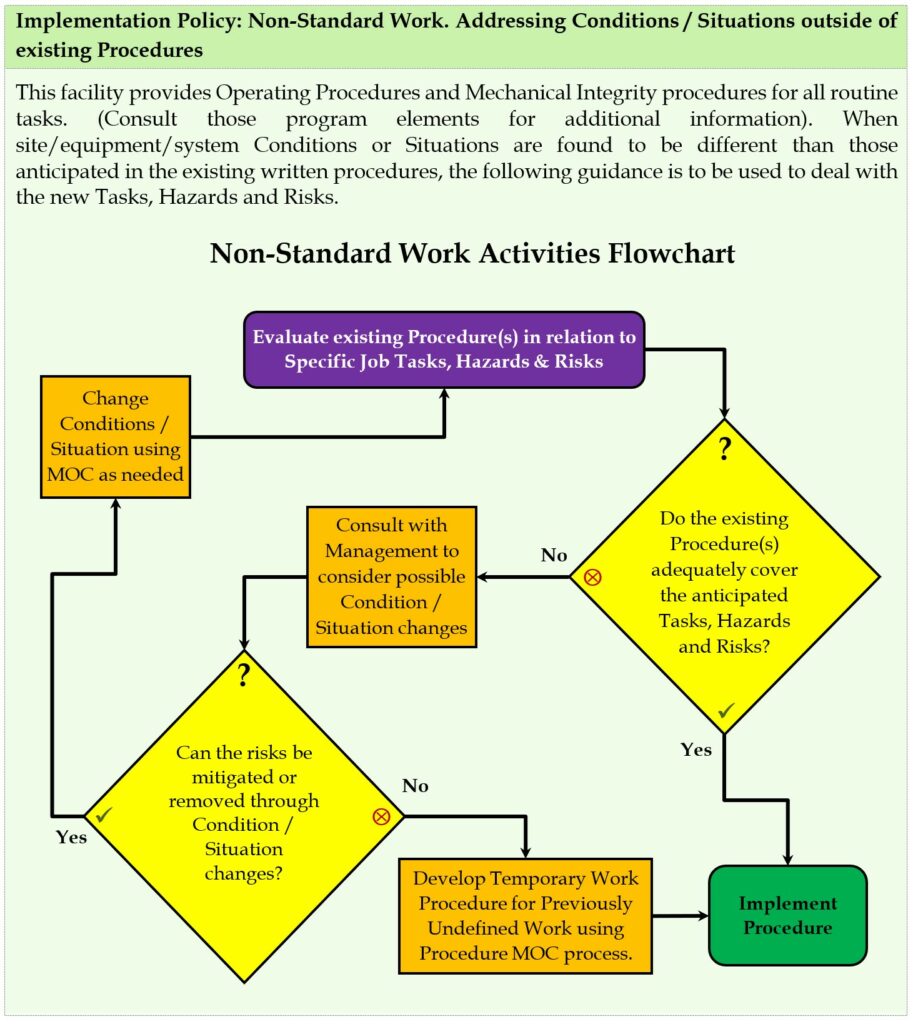
To ensure integration of this policy, the following text was added to the Operating Procedures (Implementation Policy: Using an SOP – Performing a Procedure, and Implementation Policy: Operating Phases, Temporary Operations) and Mechanical Integrity (Implementation Policy: Mechanical Integrity Procedures or MIPs) element Written Plans: “The Implementation Policy: Non-Standard Work. Addressing Conditions / Situations outside of existing Procedures found in the RMP Written Plan should be used when site/equipment/system Conditions or Situations are found to be different than those anticipated in the exiting written procedures.”
Are you handling non-standard / non-routine work well in your Process Safety program? If you are, and have a better idea, we’re always open to improvements. If you aren’t handling it well, perhaps you can implement the example above?
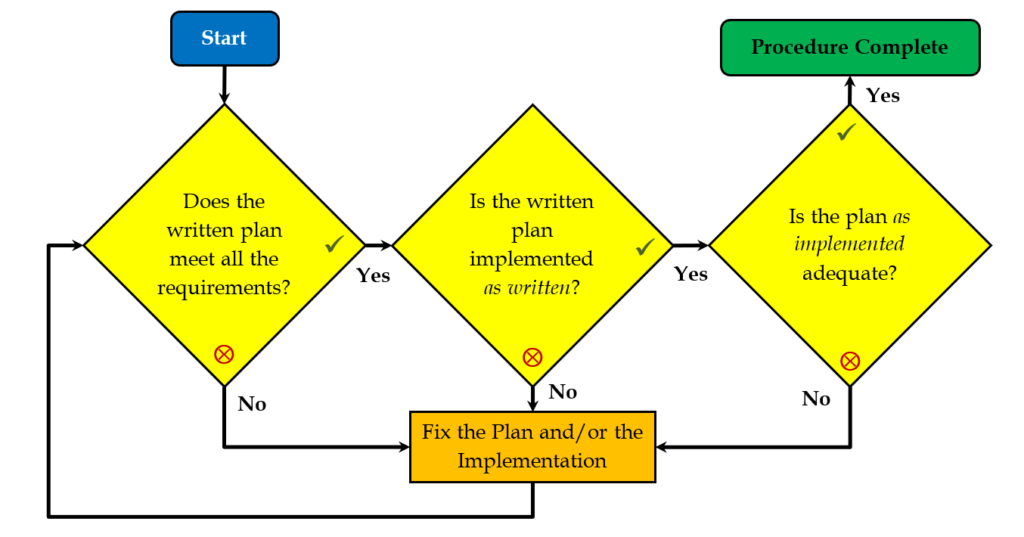
For Inside-Baseball type people: This chart was inspired by the API RECOMMENDED PRACTICE 2201 Safe Hot Tapping Practices in the Petroleum and Petrochemical Industries, Chapter 4, Section 4.3.1, Figure 3—Example Decision Process for Authorizing Hot Tapping. Other than genericizing that flowchart to cover all types of work, I also made two large changes:
- Routed the post “change conditions” step back to the start so we re-evaluate the existing procedure considering changed conditions/situations rather than short-circuiting back to the Management step.
- Rewrote the flow/wording so that Condition Changes are preferred over mere procedural changes. The thinking was that we should prefer more engineering-type changes over administrative ones, where possible.